
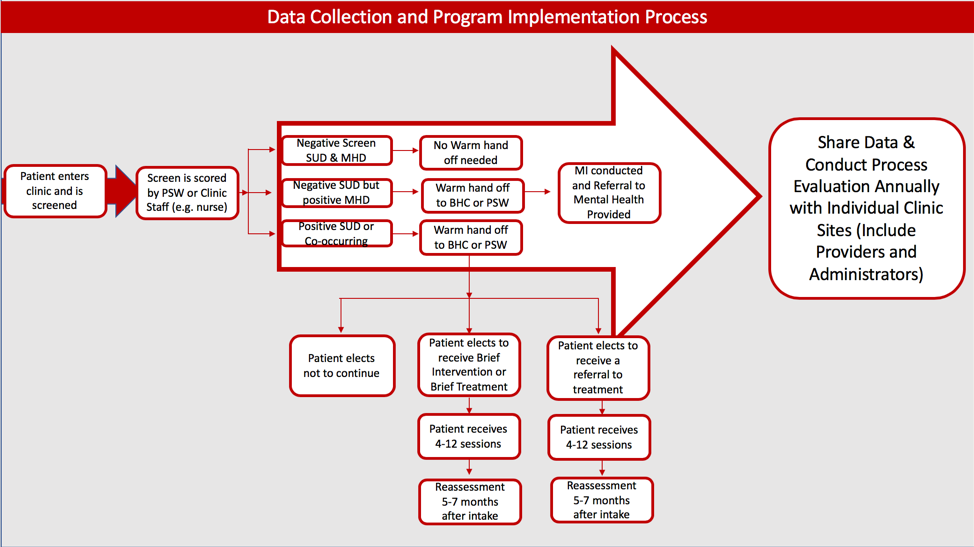
Hi! I’m Sindy Bolaños-Sacoman, Evaluator and President of SBS Consulting in the State of New Mexico. As a contractor with the University of New Mexico’s School of Medicine Department of Psychiatry and Behavioral Sciences, we just completed a five-year evaluation on a SAMHSA funded SBIRT project. We collaborated with several primary care, urgent care, tribal health centers, and trauma hospitals throughout the state. The first set of data collected was a 13-question universal screen. The screen was based on the following assessment tools: 1) Audit, 2) Drug Abuse Screening Test (DAST), 3) Primary Care PTSD Screen (PC-PTSD), and 4) Generalized Anxiety Disorder (GAD) scale. We also collected the GPRA data. The program integrated behavioral health services through a Behavioral Health Counselor and a Certified Peer Support Worker (CPSW) in medical settings. The figure below reflects the flow of the screening and referral process used.
Lessons Learned:
- Universal screening can help identify patients who are unaware, yet in need of, behavioral healthcare services, substance abuse treatment, or treatment for co-occurring mental and substance use disorders.
- Mental Health conditions are no different than physical health conditions and should be screened in the same manner.
- Peer Support Workers help bridge a gap through shared experiences, gained trust, decreased stigma and discrimination; and their involvement led to same-day revised screen data when patients opened up about actual substance use behaviors.
- Data collected and shared with healthcare sites improved healthcare delivery, increased the number of clients who obtained behavioral health services, increased awareness of substance use and abuse among unexpected populations (e.g. an elderly female presenting for a physical or a cold), and increased awareness among physicians of the variety of populations with unidentified behavioral health and/or substance use problems.
- Physicians are more comfortable asking patients about substance use and behavioral health when they have a Peer Support Worker and a Counselor to whom they can provide a warm hand off. Physicians reported improved patient overall wellbeing, self-care, and adherence to medical treatment plans.
- Patients screened in rural clinical settings were less willing to receive treatment.
Hot Tips:
- Place high priority on what and how data will be used. Screening for anxiety, trauma, and depression in addition to substance use was vital.
- Share data with stakeholders and conduct process evaluation. Collect process data whenever possible to help tell your story and obtain buy in. Many health benefits and behavior modifications that occurred, with both patients and medical staff, were identified through process evaluation. Providing a one-page summary of individual clinic data limited selection bias and increased support for SBIRT by medical providers.
- Implementation of a universal screen minimized provider bias and provided a representative sample. For many patients who screened positive, providers admitted that they would not have asked about substance use or behavioral health based on physical characteristics (age, gender, employment, etc.).
- Sharing data with the stakeholders about the benefits of Peer Support Workers; universal screening; and the need for inclusion of anxiety, trauma, and depression in a substance abuse screen led to new state Medicaid billing codes.
The American Evaluation Association is celebrating Behavioral Health (BH) TIG Week with our colleagues in Behavioral Health Topical Interest Group. The contributions all this week to aea365 come from our BH TIG members. Do you have questions, concerns, kudos, or content to extend this aea365 contribution? Please add them in the comments section for this post on the aea365 webpage so that we may enrich our community of practice. Would you like to submit an aea365 Tip? Please send a note of interest to aea365@eval.org. aea365 is sponsored by the American Evaluation Association and provides a Tip-a-Day by and for evaluators.
I agree that mental health conditions should receive the same health screening as physical health conditions. Your lessons learned were very interesting, especially in the increased awareness of substance use and abuse among unexpected populations and the increase in the variety of people being treated with unidentified mental health issues.